31
Oct
Nursing documentation is an attempt to present the. Nursing documentation is an attempt to present the.
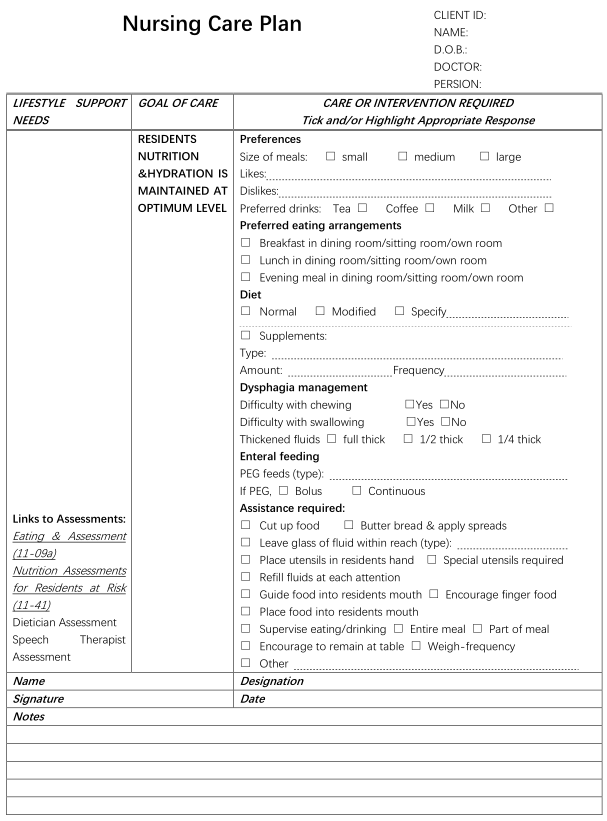
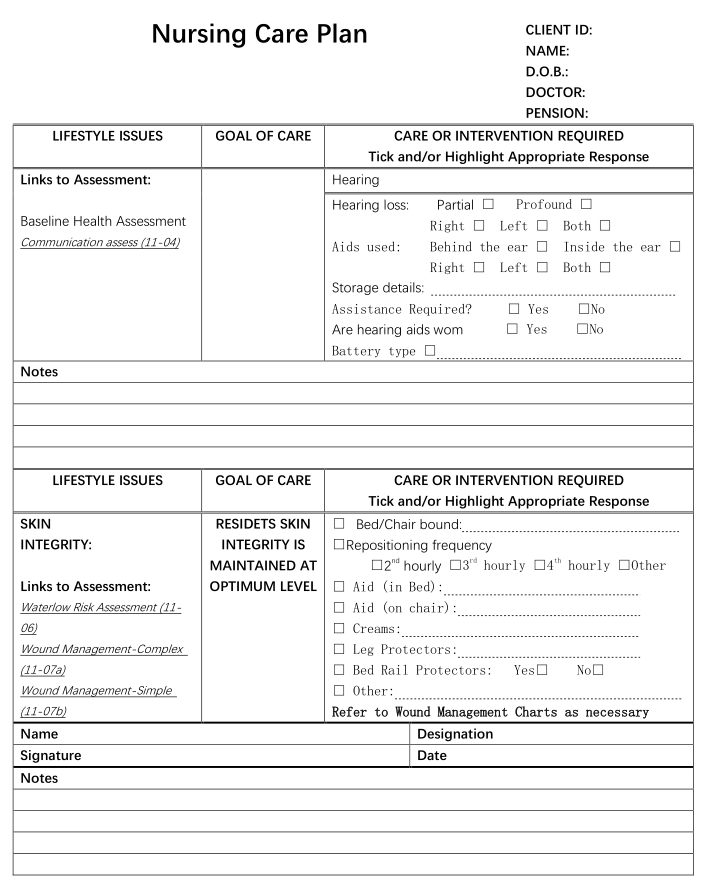
Documentation in aged care nursing. Documentation Skills in Aged Care - Progress Notes Overview Each client who is receiving aged care assistance must have a Care Plan in place to ensure on-going care needs are met. Progress Notes contribute to the review and updating of Care Plans to ensure these care needs are adequate. Nursing Documentation in Aged Care.
A Guide to Practice challenges nurses to regard quality documentation as a reflection of quality care. Good documentation is presented as the key to evidencenot only for legal and regulatory purposes but also for improved professional practice. Evidence of quality leads to expanded knowledge and provides a rich fertile ground for future.
Nurses in aged care sense that increasing documentation demands are drawing them further away from direct care. The scope of this activity and its impact on nursing workload in aged care facilities and more importantly the time Ôleft overÕfor direct patient care with older people who have more complex care needs Palmar. In residential settings documentation assists aged care facilities to receive appropriate funding for an individual from government agencies.
Progress notes act as a measure of the care needs of residents allowing resident dependency to be correctly assessed. It is important that changes in the individual consumer are recorded so that correct subsidy levels can be accessed. To develop an Australian nursing documentation in aged care Quality of Australian Nursing Documentation in Aged Care QANDAC instrument to measure the quality of paper-based and electronic resident records.
The instrument was based on the nursing process model and on three attributes of documentation quality identified in a systematic review. Feb 14 2020 - Explore Karina Marzullos board Nursing documentation examples on Pinterest. See more ideas about nursing documentation nursing documentation examples nursing notes.
Nursing documentation has been defined as the record of nursing care that is planned and given to individual patients and clients by qualified nurses or by other caregivers under the direction of a qualified nurse Urquhart et al. Nursing documentation is an attempt to present the. Nursing documentation is the record of nursing care that is planned and delivered to individual patients by qualified nurses or other caregivers under the direction of a qualified nurse 1.
Nursing documentation is the principal clinical information source to meet legal and professional requirements 2. Documentation and management of health care records. All health care personnel who document or manage health care records must be provided with appropriate orientation and ongoing education on the documentation and management of health care records.
The content and delivery of education programs should be informed by health care record audits. Documentation can be paper-based electronic or a mix of both. It can also take a number of forms including the care plan handover notes checklists pathology results operation reports and discharge summaries.
For this criterion organisations are required to have in place systems to ensure that essential information about a persons care is documented in the healthcare record. CRM Nursing Documentation System help in developing a business strategy for NDIS and Aged Care. A number of studies assessing the effects of these systems on nursing work have been conducted in hospitals and their focus has mainly been on time spent on activities by nursing staff.
For example six months after the implementation of an electronic documentation system in an intensive. Nursing documentation is often seen as a tiresome chore - although this is an understandable view the reality is that in addition to meeting ethical and other professional requirements the good. The purpose of nursing documentation is to communicate health information facilitate quality assurance and research demonstrate nurses accountability and.
The quality of nursing documentation is an important issue for nurses both nationally and internationally. Nursing documentation should but often does not show the rational and critical thinking. The implementation of electronic systems in aged care homes was anticipated to improve documentation quality.
Standardized nursing terminologies developed to improve communication and advance the nursing profession are not required in aged care practice. The language used by nurses in the nursing care plan and the effect of the electronic system on documentation quality in residential aged care. To optimise the efficiency benefit of electronic documentation in a residential aged care facility it is not only necessary to automate all nursing forms but also to ensure that the system is aligned with caregivers documentation practice.
Continuous education and mentor support is essential to ensure caregivers effective usage of the electronic system. Nursing documentation for communicating and evaluating care The results of this study can provide a part of a basis upon which a multi-professional patient record could be developed and which could also function as an alarm to managers at different levels to prioritize the.
Previous post
Does ampicillin have penicillin in itNext post
Doctor de cabecera english